Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
ZAPOROZHYE STATE MEDICAL UNIVERSITY CHAIR OF HOSPITAL SURGERY ASSISTANT PROFESSOR KLYMENKO A.V. LOWER EXTREMITY PERIPHERAL ARTERIAL DISEASE (LEPAD) 1 пятница, 5 сентября 2003 г.
 1 пятница, 5 сентября 2003 г.")
2
LEPAD Atherosclerosis Buerger Disease (Thromboangiitis Obliterans) Takayasu Arteritis (Non-specific aortoarteritis) Combinations
 Takayasu Arteritis (Non-specific aortoarteritis) Combinations")
3
Classification of cronic ischaemia by Fonthen - Pokrovskiy I degree: asymptomic – ischaemia of tension – parastesia, numbness, extremity coldness II degree: intermittent claudication А – more than 200 m of walking В – less than 200 m of walking III degree: rest pain, night pain. IV degree: necrotic changes – necrosis, gangrene, ulcer.

4
:12 Occlusion\stenosis level Aortal-ileal segment – aorta lower than renal arteries till external ileac artery at inguinal ligament. Femoral-popliteal segment – common, superficial and profunda arteries, popliteal artery till its threefurcation. Periferal (distal) segment – shin arteries ( anterior and posterior thibial arteries).

5
:12 Points for auscultation of the arteries

6
:12 Normal angiography

7
:12 Aortal-ileal segment

8
:12 Femoral-popliteal segment

9
:12 Periferal (distal) segment
 segment")
10
:12 BACKGROUND Atherosclerosis is the leading cause of occlusive arterial disease of the lower extremities Atherosclerosis is also a leading cause of death and disability in the developed world Atherosclerotic lesions affect large and medium-sized arteries

11
PATHOPHYSIOLOGY STAGES 1) a fatty streak 2) a fibrous plaque 3) a complicated lesion
 a fatty streak 2) a fibrous plaque 3) a complicated lesion")
12
a fibrous plaque Chronic ischaemia ATHEROTHROMBOSIS ruptureDevelopping of the thromb The thromb encloused into atheroma Stableplaque Emboli Occlusion Acute ischaemia Acute ischaemia

13
THEORIES Hypercholesterinaemia Dislipidaemia Infective Macrofagal Lipid peroxide Traumatic

14
RISK FACTORS Hyperlipidaemia Tobaco smocking Fat body Hypodynamia Stress Diabetis melitus Hypertony Age more then 45

15
FREQUENCY In the US: on the basis of ancle-brachial blood pressure ratios, the prevalence of LEPAD is approximately 3% in people younger than 60 years. The prevalence increases to 20% in people older than 70 years.

16
Mortality \ Morbidity The mortality rate in patients with LEPAD is 6 times higher than that of age-matched control subjects, and it is almost exclusively the result of death due to myocardial infarction and stroke. The 10-year survival rate decreases from 80% to 55% in healthy individuals compared with patients with symptoms of LEPAD

17
RACE No racial predilection exists for the development of LEPAD

18
SEX Males and females have an equal risk of LEPAD; however, atherosclerosis of the lower extremities is seen most frequently in elderly men.

19
AGE The highest incidence occurs in those aged years

20
Preferred examination Ankle-brachial index Plethysmography Doppler ultrasonography Conventional arteriography Computed tomography angiography and magnetic resonance angiography

21
Doppler ultrasonography

22
Stenosis of the profundal femoral artery Doppler ultrasonography.

23
:12

24
Conventional arteriography

25
:12 Conventional arteriography

26
:12 Occlusion of the trifurcation of the popliteal artery

27
:12 Occlusion of the thibial arteries

28
:12 CLINICALY IV degreeIII degree

29
:12 Spasmolytics: papaverin, No-spa, nicotin acid Decreasing of thrombotic activity: heparin, fractioned heparin, sincumar Antiagregants: aspirin, trental, ticlid, ipaton Metabolics: vit. E, vit A, esenciale Metabolics improoving oxidation: solcoseryl, actovegin Hypolipidaemic: lovostatin, liprimar Enelbin MEDICINESMEDICINES

30
ACTION OF ANTITHROMBOSITICS

31
:12 AORTABIFEMORAL SHUNTING PROSTHESIS AORTA

32
:12 Reimplantation of the inf. mesenteric artery into the prosthesis inf. mesenteric artery prosthesis

33
:12 After the ABSh

34
Endarterectomy out of the femoral artery

35
Endarterectomy plus autovenous profundoplasty

36
Femoral-popliteal shunting with artificial graft

37
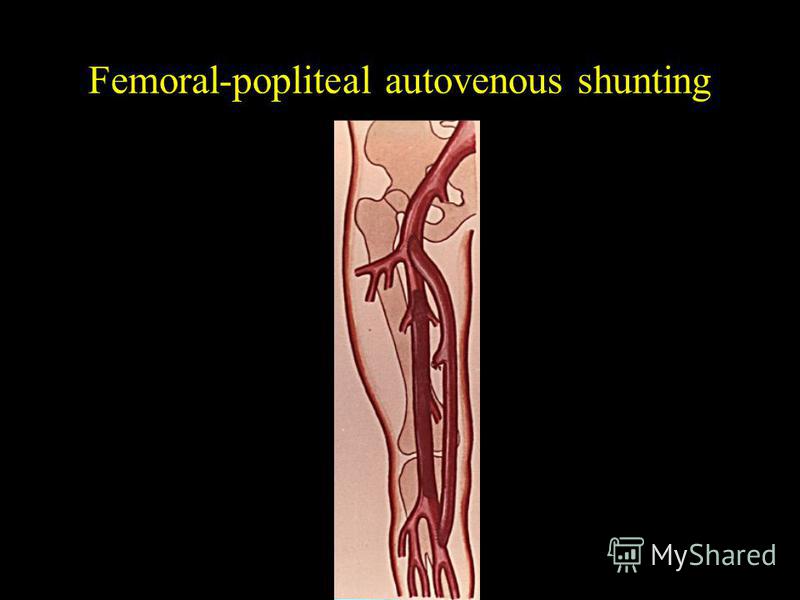
Femoral-popliteal autovenous shunting

39
Balloon angioplasty plus stenting before after

40
Buerger Disease (Thromboangiitis Obliterans) Rare Distal segment in 70% It can be in remission and exacerbation Stages: - prodromal - angiospastic - angiotrofic - gangreenous
 Rare Distal segment in 70% It can be in remission and exacerbation Stages: - prodromal - angiospastic - angiotrofic - gangreenous")
41
Buerger Disease (Thromboangiitis Obliterans) It begins at allergic reaction with primery or secondary angiospasm, which makes hypoxia and blood flow decreasing. After that there will be immune inflamation with endotelial proliferation fand thrombosis. Medicamental treatment is preferable. In case of complication you may use sympatectomy and amputations.
 It begins at allergic reaction with primery or secondary angiospasm, which makes hypoxia and blood flow decreasing. After that there will be immune inflamation with endotelial proliferation fand thrombosis")
Еще похожие презентации в нашем архиве:







 was established in 1948 to provide high-quality free medical treatment.")










, I (for infectious) and R (for recovered). Therefore, this.")