Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
OCCUPATIONAL EXPOSURES TO BLOOD AND BODILY FLUIDS Dr Chow TS Infectious Disease Unit Medical Department HPP

2
Scope Bloodborne pathogens HIV Hep B Hep C Others: Malaria, syphilis, HTLV-1 etc. Assessment Management per protocol Prevention

3
INFECTIOUS Body fluids containing visible blood Semen Vaginal secretions CSF Synovial fluid Pleural fluid Peritoneal fluid Pericardial fluid Amniotic fluid Tissue NOT INFECTIOUS Unless contaminated with blood Feces Nasal secretions Saliva Sputum Sweat Tears Urine Vomitus

5
Needle stick injury occurred …. Recapping of needle Insertion of branulas Sticking used needles onto mattress (very common in AE) Not using sharp bin and blood taking trolley appropriately Overflow of sharp bin Carelessness during procedures e.g. CVL etc Not using glove during procedure Needles that were not disposed properly
 Not using sharp bin and blood taking trolley appropriately Overflow of sharp bin Carelessness during procedures e.g. CVL")
6
Overflow of Sharp Bin

7
IMPROPER DISPOSAL OF WASTE - AVOIDED Needle and sharps being discarded inappropraitely

8
Needles being thrown into the sink

9
Needles being thrown onto the floor

10
Weird situations… Needles in general waste Needles in tissue box (made into sharp bin by HO) Needles in boxes (needle being used as scissors to cut tape on the box in store) Needles on the mattress of bed (very common) Needles on the drip set
 Needles in boxes (needle being used as scissors to cut tape on the box in store) Needles on the mattress of bed (very common) Needles on the drip set")
11
Is it important to know how it occurred ? Yes, study the pattern of injury will give us some information for remedial measures to be taken.

12
POST OFFICE HOURS - ED MANAGEMENT AFTER Occupational exposures POST OFFICE HOURS - ED

13
Post exposure management First aid Serological testing Counseling Immunoprophylaxis/ vaccine/ antiviral/anti infectives

14
FIRST AID after exposure - HCW IMMEDIATE MEASURES: Skin: Wash thoroughly with soap & water Eye: Rinse thoroughly with sterile saline, clean water flush Mouth, Nose: Clean water rinse/flush No evidence that using antiseptics/ disinfectant or expressing fluid by squeezing the wound further reduces risk SEEK ADVICE EARLY Preferably prophylaxis should be commenced within 1 –2 hrs of the exposure

15
Report the incident- HCW Sister on call Consultant / specialist / MO in charge if not sure of what to do Fill up incident form HPP/QUA/BR-08-pindaan1 Form IR1 (will be submitted by respective ward/unit to QA the next working day after HOD signed)
")
16
Report to infection control unit and take forms from ward/ place of incident Call Sister Hafizah (on call 24 H) for assistance if in doubt. Other wise : need to ask the exposed HCW to notify to IC unit in ACC the next working day To fill up OHU SIS-1 (exposed HCW), OHU-SIS 2a, OHU SIS – 2b (attending ID physician) EPINet form (Exposed HCW)
 for assistance if in doubt. Other wise : need to ask the exposed HCW to notify to IC unit in ACC the next working day To fill")
17
Refer ED MO after office hour Initial assessment to be done by ED MO, Call 7030/ ID consultant on call to discuss further if in doubt. What assessment to be done? Serology testing Counseling Antiviral / immuno-prophylaxis Follow up arrangement

18
Blood taking – ward of incident Fill up PER PAT 301 form in 2 : 1 for Source patient (details and diagnosis) 1 for HCW, write SHARP INJURY on both forms Informed consent to be taken for both source and HCW (by respective ward Dr) Take 5 ml blood in red tube each, Source: HIV, HepBsAg, HCV HCW: HIV, HepBsAg, Anti Hep Bs Ab, HCV If source or HCW refused HIV testing – no HIV test to be done. VDRL – not routine
 1 for HCW, write SHARP INJURY on both forms Informed consent to be taken for both source and HCW (by respective ward Dr) Take 5 ml blood in r")
19
Blood sampling- HCV source If source is known/diagnosed HCV positive: send source patient and HCW blood for HCV RNA PCR tests to HSB ( as baseline) in 2 tubes EDTA /purple/FBC tube for both samples. Fill up PER PAT 301 form with full history
 in 2 tubes EDTA /purple/FBC tube for both samples. Fill up PER PAT 301 form with full history")
20
Serology Testing – send from ED Send both tubes of samples (HCW and SOURCE) with PER PAT 301 forms (X2) and the HCW to ED ED MO need to fill up Sharp injury Form HPP (HPP/PAT/MM/QP/013-APPENDIX 1) contact number of the ED MO who attended the case IS NEEDED Informed the lab 5153, 5152 after office hour to run rapid test HIV and Hep B for both source and HCW immediately The lab will call you back once result is out.
 with PER PAT 301 forms (X2) and the HCW to ED ED MO need to fill up Sharp injury Form HPP (HPP/PAT/MM/QP/013-APPENDIX 1) contact number of the ED MO who attended the case IS")
21
Information needed: ED MO to take HCW details: years of service, unit involved Date, time and location of the exposure Details of the procedure being performed and the use of protective equipment at the time of the exposure The type, severity, and amount of fluid to which the HCW was exposed HCW Vaccination history (Hep B) Lady HCW: pregnant? Details about the source patient ( high risk for HIV, HCV or HBV?) – need the input from respective ward MO

22
Trace the result within 1 Hour…HIV If the source is HIV negative by rapid test: no PEP If the source is HIV negative but has high risk of HIV – may consider PEP High risk: unprotected sexual exposure with multiple partner, MSM, IVDU, partner of known HIV patient: may start PEP If HIV status unknown (unknown source or soucre refused to be tested) : may consider PEP depending on circumstances If HIV positive : call ID consultant and start extended regime PEP. PEP: COMBIVIR 1 tablet 12 hourly Extended : COMBIVIR + KALETRA 2 tablet 12 hourly

23
DETAILS OF HIV EXPOSURES

24
Main determining factors : HIV exposure Infective source (HIV Status ): HIV viral concentration, volume of specimen involved in exposure, clinical stage, CD4 cell count, current antiretroviral therapy, etc. Level of Exposure (Exposure Severity): Depth of injury, instrument involved, duration of exposure, integrity of skin/mucous membranes.
: HIV viral concentration, volume of specimen involved in exposure, clinical stage, CD4 cell count, current antiretroviral therapy, etc. Level of Exposure (Exposure Severity): Dept")
25
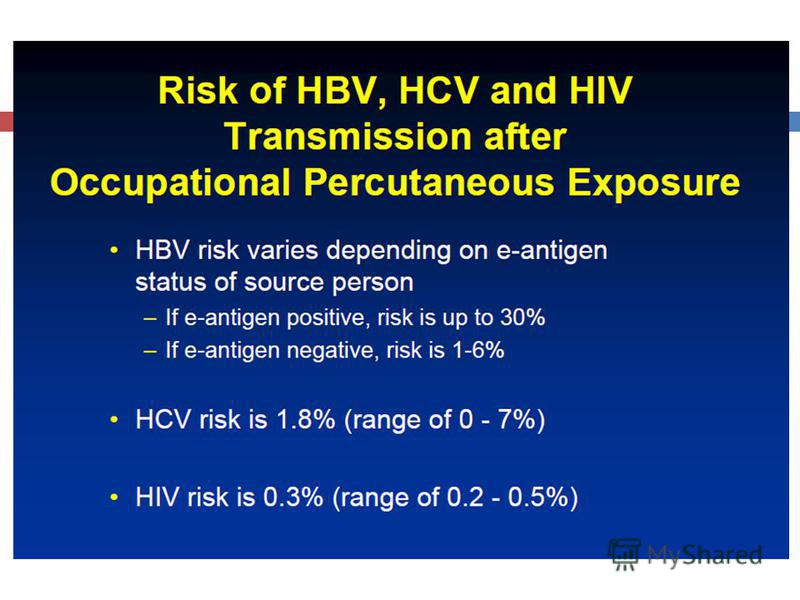
Risk of HIV Transmission 1. Bell DM. Am J Med 1997;102(suppl 5B):9-15.
:9-15.")
26
Recommended HIV PEP for percutaneous injury Exposure type Asymptomatic HIV Low VL Symptomatic HIV High VL Status Source Unknown Unknown source HIV negative Less severe (solid needle/ superfi inj 2 drug PEP Expanded 3 drug PEP Gen. no PEP. Consider 2 drug for high risk Gen. no PEP. Consider 2 drug in high risk setting No PEP More severe (Large bore, deep Expanded > 3 drug PEP Expanded 3 drug PEP Gen. no PEP. Consider 2 drug for high risk Gen. no PEP. Consider 2 drug in high risk setting No PEP

27
Recommended HIV PEP for mucous membrane & non-intact skin Exposure type Asymptomat ic HIV Low VL Symptomatic HIV High VL Status Source Unknown Unknown source HIV negative Small vol. (few drops only) Con. 2 drug PEP R. 2 drug PEP Gen. no PEP. No PEP Large vol. (Major blood splash) R. 2 drug PEP R. Expanded 3 drug PEP Gen. no PEP. Consider 2 drug for high risk Gen. no PEP. Consider 2 drug in setting No PEP
 Con. 2 drug PEP R. 2 drug PEP Gen. no PEP. No PEP L")
28
Tolerability of HIV PEP in Health Care Workers Percent of HCWs Wang SA. Infect Control Hosp Epidemiol 2000;231: Incidence of Common Side Effects

29
WHEN SHOULD PEP BE STARTED?

30
Timing of PEP: CDC Guidelines PEP should be initiated as soon as possible, preferably within hours rather than days of exposure. Interval after which there is no benefit for humans is not known Obtain expert advice when interval has exceeded hours MMWR 2005;54(No. RR-9).

31
Duration of PEP 4 weeks (28 days) used in case-control study 2 and recommended by CDC guidelines 3 1. Tsai C-C et al. J Virol 1998;72: Cardo DM et al. NEJM 1997;337: MMWR June 29, 2001:50(RR11);1-42.
 used in case-control study 2 and recommended by CDC guidelines 3 1. Tsai C-C et al. J Virol 1998;72:4265-73. 2. Cardo DM et al. NEJM 1997;337:1485-90. 3. MMWR June 29, 2001:50(RR11);1-42.")
32
PEP Regimens: Basic regimens Latest guidleines Two NRTIs Simple dosing, fewer side effects Preferred basic regimens: CDC 2009 Combivir (Zidovudine 300 mg+ Lamivudine 150 mg) 1 tab BD for 4 weeks or Tenvir –EM ( Tenofovir 300 mg + Emtricitabine 200 mg) 1 Tab OD for 4 weeks
 1 tab BD for 4 weeks or Tenvir –EM ( Tenofovir 300 mg + Emtricitabine 200 mg")
33
Expanded PEP Regimens Basic regimen plus a third agent Rationale: 3 drugs may be more effective than 2 drugs, though direct evidence is lacking Consider for more serious exposures or if resistance in the source patient is suspected Adherence more difficult More potential for toxicity

34
Expanded PEP Regimens Preferred Expanded Regimen: For 28 days CDC 2010 *Atazanavir requires ritonavir boosting if used with tenofovir Combivir 1 tab 12H + Kaletra 2 tab 12 H Tenvir EM 1 tab OD + Kaletra 2 tab 12 H

35
Adverse Effects: Basic vs Expanded Regimens % of individuals Puro V et al. 9th CROI, February 2002, Abstract 478-M

36
Follow-up of (HCW) exposed to known or suspected HIV-positive sources Exposed HCW should be advised to use precautions (e.g., avoid blood or tissue donations, breastfeeding, or pregnancy) to prevent secondary transmission, especially during the first 6–12 weeks post-exposure. For exposures for which PEP is prescribed, HCW should be informed regarding: need for monitoring (F/U serology tests: HIV serology, HBsAg, HCV serology 0, 6 weeks, 3 and 6 months) Monitor side-effects if given antiretroviral drugs: Symptoms: GI upset, malaise, myalgia Laboratory: FBC, LFT, RP possible drug interactions (OCP, anti epileptic, warfarin) the need for adherence to PEP regimens. Consider re-evaluation of exposed HCW 72 hours post-exposure, especially after additional information about the exposure or SP becomes available. MMWR 2005;54(No. RR-9).
 exposed to known or suspected HIV-positive sources Exposed HCW should be advised to use precautions (e.g., avoid blood or tissue donations, breastfeeding, or pregnancy) to prevent secondary transmission, especially during the first")
37
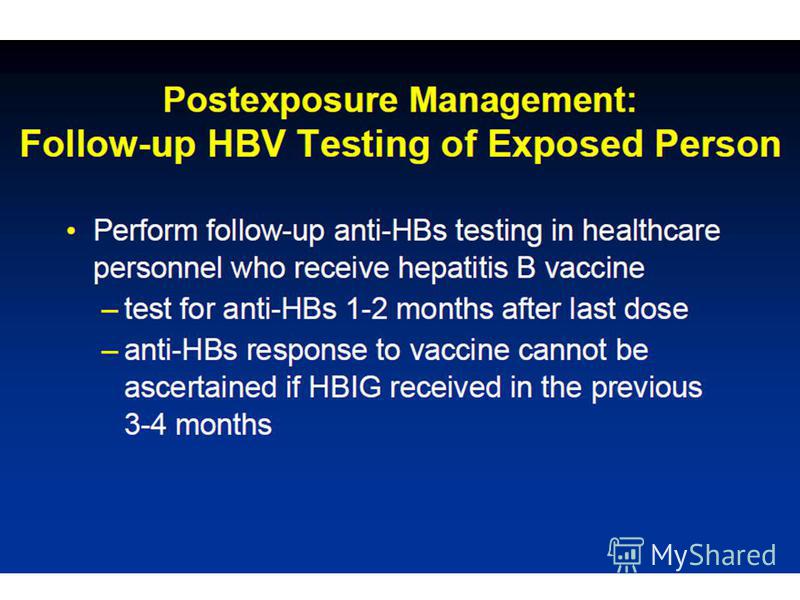
Follow-up HIV Testing CDC recommendations: HIV Ab testing for 6 months post-exposure (e.g., at 6 weeks, 3 months, 6 months) Extended HIV Ab testing at 12 months is recommended if health care worker contracts HCV from a source patient co-infected with HIV and HCV VL testing not recommended unless primary HIV infection (PHI) suspected MMWR 2005;54(No. RR-9).
 Extended HIV Ab testing at 12 months is recommended if health care worker contracts HCV from a source patient co-infected with")
38
PEP for HIV in pregnant HCW Decision is drawn after discussion with HCW Do not deny PEP solely on the basis of pregnancy Efavirenz not recommended Combivir +/- Kaletra

39
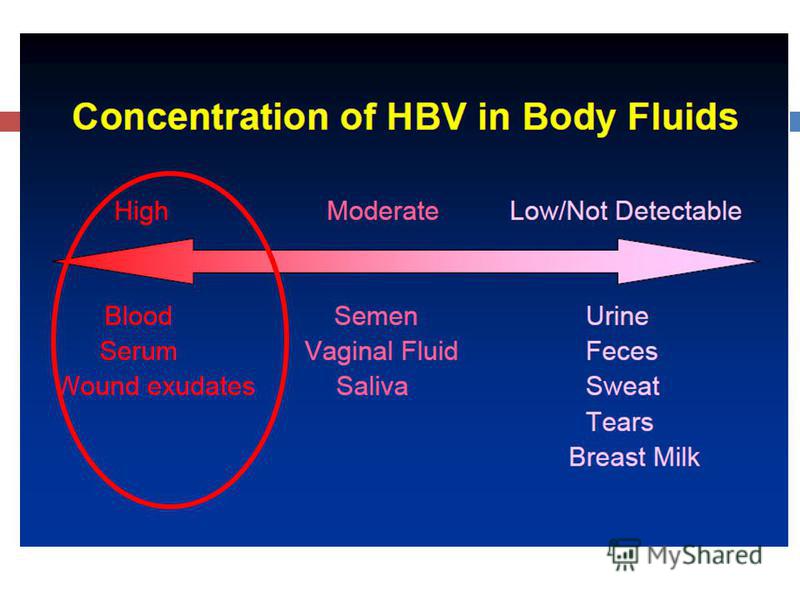
OCCUPATIONAL HBV EXPOSURES

43
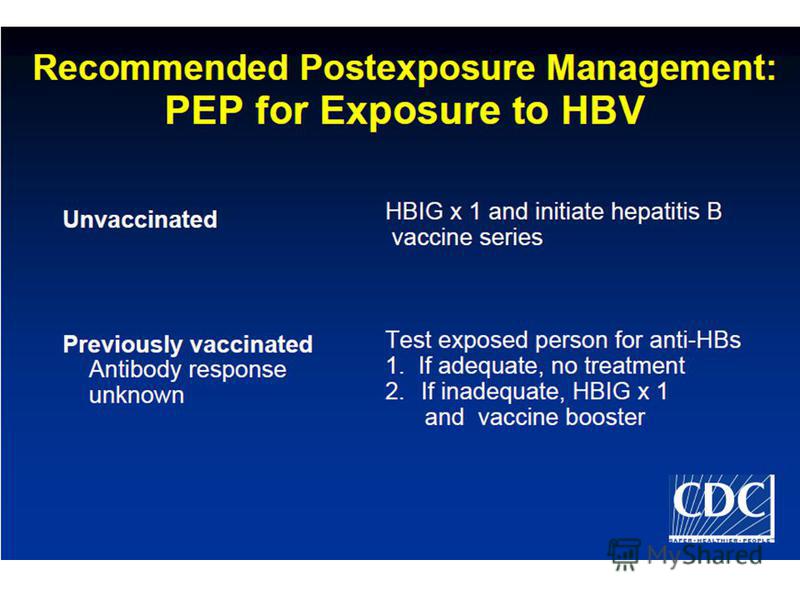
Trace result within 1 hour - HBV If source blood rapid test for Hep Bs Ag is negative: no need PEP for HBV If source blood rapid test is Hep BsAg + ve: HCW vaccinated with 3 doses and sure Hep B s Ab level tested before was > 10 IU/ml= no need PEP HCW not vaccinated or unsure of vaccination/antibody level: use IM immunoglobulin Ig G (immuno-prophylaxis) Then later Hep B booster/revaccination

47
DOSE: HBIG A single dose of HBIG (0.06 ml/kg or 5.0 ml for adults) should be given as soon as possible after exposure and within 24 hours if possible. HB vaccine 1 ml (20 ug) should be given IM at a separate site as soon as possible, but within 7 days of exposure, with the second and third doses given 1 month and 6 months, respectively, after the first HBIG
 should be given as soon as possible after exposure and within 24 hours if possible. HB vaccine 1 ml (20 ug) should be given IM at a separate site as soon as possible, but within 7 day")
48
OCCUPATIONAL HCV EXPOSURES

49
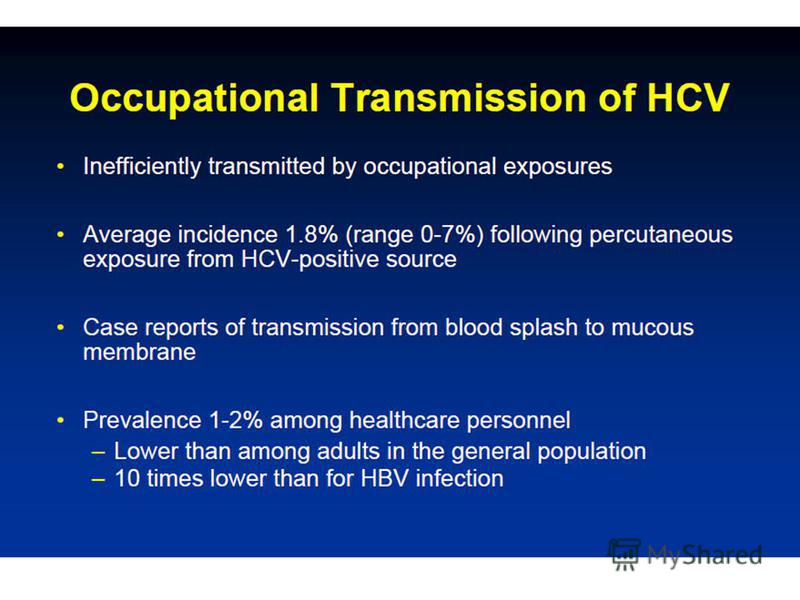
Trace result HCV - If source HCV known +ve: need to send HCV RNA for source and HCW in pair to HSB Use 2 bottle EDTA each If source unknown or negative : nothing to be offered as PEP, just give FU date.

52
Hep C exposure If source is confirmed HCV positive: HCW negative for HCV HCW and the source blood need to be taken for HCV RNA (detectable in 1-3 weeks post exposure) HCV antibody (90% who seroconvert will do so in the first 3 months) NO reccomended prophylaxis Monitor early infection HCW who remained HCV RNA detectable 8-12 weeks post exposure will need a course of Pegylated IFN Gastro 130: 2006
 HCV antibody (90% who seroconvert will do so in the first 3 months) NO reccomended")
53
OTHERS

54
Other possible pathogens Malaria: 1 HO had needle stick injury past 3 weeks, exposed to Vivax Malaria patient 2 weeks later developed high swinging fever, HO suspected malaria via needle stick transmission HO BFMP turned out to have Vivax Malaria!! CDC recorded only 1 case transmission (falciparum) – very rare but could occur No post exposure prophylaxis recommended Need to watch out and high index of suspicion

55
Syphilis If incident of syphilis is high Source is having active primary or secondary syphilis (chancre or rash) Test for VDRL/TPHA only indicated Exposed HCW : IM 2.4 Benzathine Penicillin stat may be given.
 Test for VDRL/TPHA only indicated Exposed HCW : IM 2.4 Benzathine Penicillin stat may be given.")
56
Dont Forget...Emotional impact! Can be severe and long lasting even when serious infection is not transmitted impact is particularly severe when the injury involves exposure to HIV, HCV. Not knowing the infection status of the source patient can accentuate the HCWs stress. (HIV and Hep B rapid test play important role) In addition to the exposed HCW, colleagues and family members may suffer emotionally.

57
Reference National Institute for Occupational Safety and Health bloodborne pathogens website Occupational Safety and Health Administration bloodborne pathogens website slc.gov/SLTC/bloodbornepathogens/index.html

58
THANK YOU!!

Еще похожие презентации в нашем архиве:






















 The virus compromises the bodys ability to handle disease and causes AIDS. AIDS~ (Acquired Immune Deficiency.")